
Lipoedema: What Is It and What Treatments Are Available?

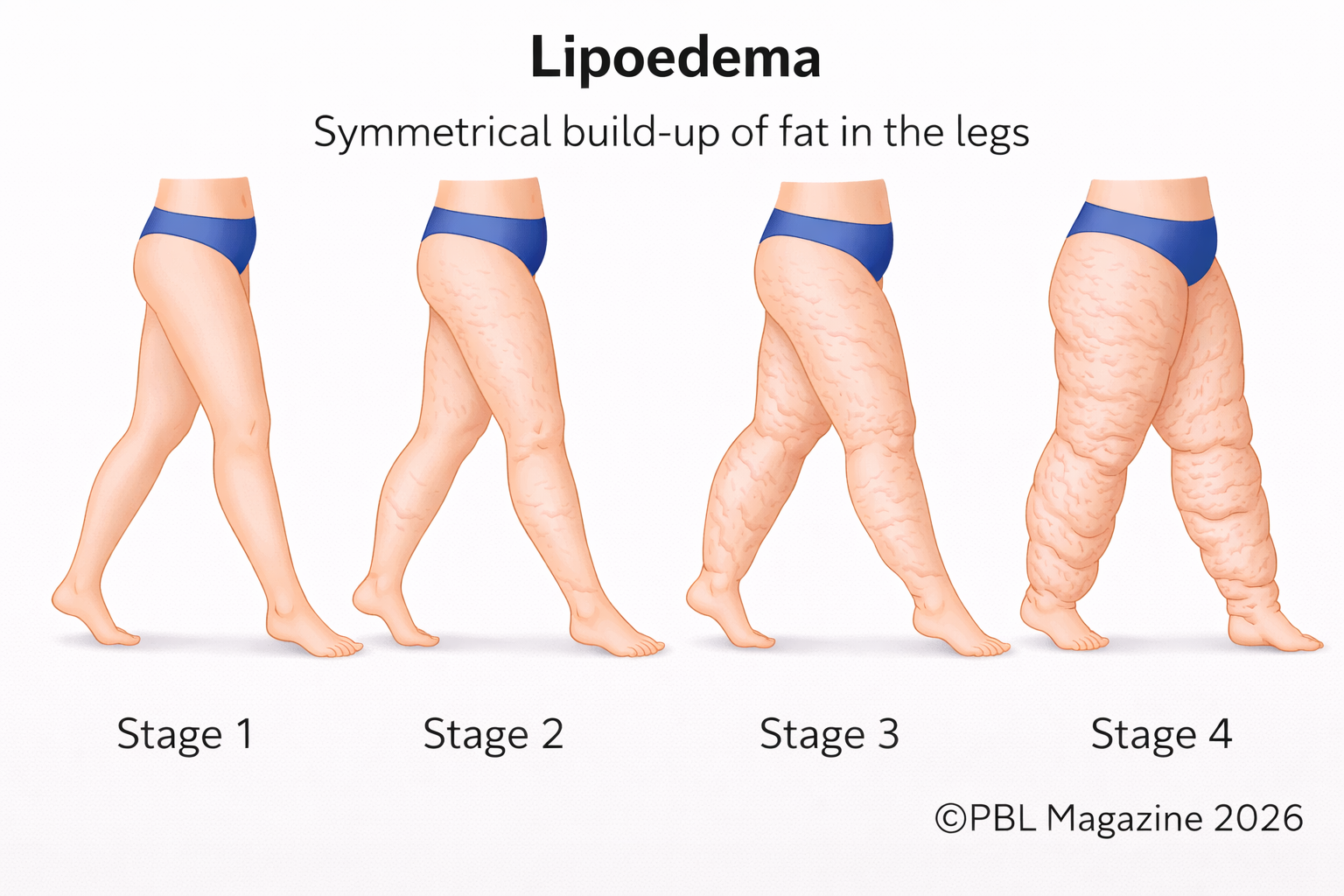
Women’s health conditions have long been shaped by delay: delayed recognition, delayed diagnosis and, in many cases, delayed research. Lipoedema is increasingly being discussed in that context, with studies suggesting it may affect around 6 to 11 per cent of women, yet it remains widely misunderstood and frequently mistaken for obesity or simple weight gain. Lipoedema is a chronic condition that affects the way fat is distributed in the body, most commonly in the legs, hips and buttocks, and sometimes the arms. It usually affects women, and is marked by a symmetrical build-up of fat that can be painful, tender and prone to bruising. The feet and hands are often unaffected, which can leave a distinct cuffing effect at the ankles or wrists. Despite this, the condition is still regularly mistaken for obesity, lymphoedema or simple weight gain.
Many women with lipoedema report years of delayed diagnosis, during which their symptoms are dismissed or reduced to lifestyle. But lipoedema does not behave like ordinary fat gain. The affected tissue is often painful, mobility can become more difficult over time, and the disproportionate fat in the limbs may not respond to diet and exercise in the way patients are told to expect. NHS guidance describes symptoms including pain, tenderness, swelling that worsens during the day, easy bruising and difficulty walking or standing for long periods.
Prevalence figures vary, largely because the condition remains under-recognised, but several reviews suggest lipoedema may affect around 6 to 11 per cent of women, with some papers placing the figure slightly higher and the NHS describes it as a “common” condition. That means it is far from rare, even if it is still poorly understood outside specialist settings.
Mr Michael Mouzakis, Consultant Plastic Surgeon at The Private Clinic which has launched a Comprehensive Lipoedema Programme, says that misunderstanding has shaped how patients are seen and how they are treated. “The inspiration for this programme is rooted in a commitment to bridging the gap between clinical pathology and patient experience. For too long, lipoedema has been misdiagnosed through a lens of lifestyle failure; my mission is to replace that stigma with evidence-based empowerment.”
Researchers do not yet fully understand what causes lipoedema, but the evidence points to a strong hormonal and genetic component. The condition often begins or worsens at points of hormonal change such as puberty, pregnancy and menopause. Family history is also commonly reported. A 2023 symptom survey involving 707 women with lipoedema found that onset was most often reported at puberty and during pregnancy, supporting the view that hormonal change plays an important role.
Lipoedema has been linked to pain, reduced mobility, difficulty with clothing, body image distress and poorer quality of life. One review citing Lipoedema UK survey data found that 87 per cent of respondents said the condition had a negative effect on their quality of life.
Mr Mouzakis describes lipoedema as “a significant, yet underserved, intersection of lymphatic health and systemic inflammation”, and says the aim should be “to advance the standard of care for a condition that is frequently ignored in traditional medical education.” His comments reflect a wider frustration among patients and clinicians that awareness has not kept pace with the burden of the condition itself.
There is no cure for lipoedema, but there are recognised ways to manage it. In the UK, NHS guidance lists healthy eating and weight management, exercise, compression, emotional support and, in some cases, liposuction as the main approaches. Conservative treatment is generally aimed at reducing discomfort, supporting mobility and limiting complications, rather than promising to reverse the condition altogether.
Compression garments are commonly used to help with discomfort and swelling. Exercise is also recommended, not because it removes lipoedema tissue, but because it supports movement, circulation and overall health. Some patients also receive manual lymphatic drainage, although the evidence for this remains less definitive than for some other aspects of care. Recent work on lipoedema research priorities identified manual treatment as one of the areas where better evidence is still needed.
For some patients, surgery may be considered. Liposuction, particularly tumescent liposuction. A 2024 meta-analysis found significant improvements after surgery in pain, oedema, bruising, mobility and quality of life. Another 2024 review reported improvements in heaviness, walking difficulty and cosmetic impairment, while also noting that many patients still require ongoing conservative care afterwards.
Mr Mouzakis sums up his approach, “It’s not your fault, but it’s your journey.” In the clinic material, he explains the aim is to “distinguish the physiological reality of adipose tissue dysfunction from the individual’s character, while simultaneously inviting the patient into an active, informed role in their own multidisciplinary care”.
That may be the most important point. Lipoedema is not simply a cosmetic concern, nor is it just a question of body size. It is a chronic condition that can affect pain, mobility, confidence and quality of life. Yet before treatment can begin, it first has to be recognised for what it is.
Mr Mouzakis says his goal is to move the patient experience “from one of systemic gaslighting to one of clinical clarity, ensuring that every woman has the diagnostic validation and the practical tools necessary to manage her health with dignity.” For many women with lipoedema, that clarity may be the thing that has been missing for the longest.







Trying to fit hair, nails, brows, lashes and tanning into the final days before a holiday can leave clients overwhelmed and salon diaries stretched. Annabelle Taurua, Beauty Expert at Fresha, shares how better planning can make the experience easier for everyone. The days before a holiday are often some of the busiest in a salon calendar. Clients want to feel polished before they travel, but many leave their appointments until the same narrow window, creating a rush that can be stressful on both sides of the reception desk.